












FUT vs. FUE
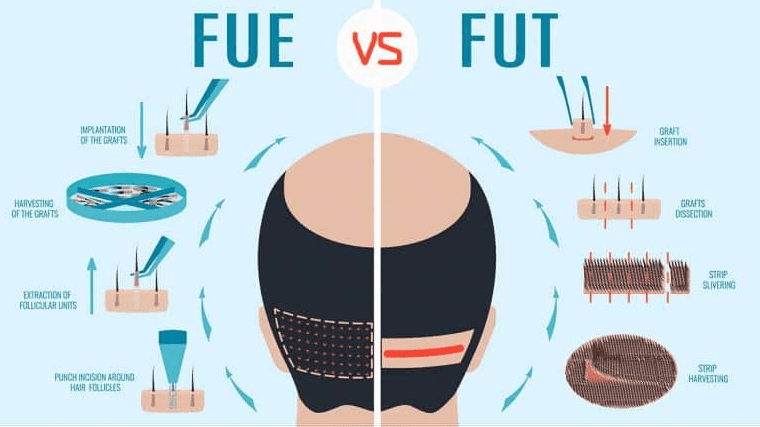
Few topics within the field of surgical hair restoration draw as much excitement and passion as the comparison between FUT and FUE. A discussion comparing the harvesting techniques typically draws ardent supporters and dissenters from each side of the aisle, and usually becomes impassioned and heated. Those who only perform FUE paint FUT as something “older” and less “advanced;” whereas those who only perform FUT are quick to point to the limitations of FUE – such as lower growth yields, more damage in the donor region, exaggerated marketing claims, and unregulated procedures. The truth of the matter is that framing the argument as FUT “versus” FUE is far too “black and white;” both techniques have merit and their place, and should be discussed and compared as synergistic adjuncts and not enemies. Those who can and do perform both FUE and FUT are generally best suited to provide unbiased information about the techniques. Patients considering whether or not they should undergo FUT or FUE should keep the following in mind:
Number of Lifetime Grafts
The number of grafts a patient can have removed from the donor area over their lifetime is finite. Patients with advanced hair loss or young patients who may progress to an advanced balding pattern must keep this in mind and treat each graft like gold. Efficient harvesting and use of these grafts is paramount to good long-term outcomes with hair transplant surgery. Beginning with FUT and utilizing strip harvesting before switching to FUE provides the greatest number of lifetime grafts. Performing subsequent strip harvests (and removing the previous scar with each new surgery so only a single incision line scar is left behind) until it is no longer advisable and then doing FUE in the areas left unutilized by strip harvesting allows patients to use their entire donor efficiently. Beginning with FUE – particularly large FUE sessions – decreases the number of grafts a patient can use from the donor area. Patients with advanced hair loss or young patients with uncertain patterns are likely best served by starting with FUT and then moving to FUE.
Growth Yield
While research is somewhat sparse and conclusions vary, the consensus of those who can perform both FUT and FUE is typically that grafts harvested via FUT grow, on average, more robust and consistently compared to those harvested via FUE. This is usually attributed to increased graft trauma inherent in the FUE extraction process and less protective tissue supporting FUE grafts during the transplant and crucial post-op period.
Donor Scarring
All hair transplant surgery creates scarring in the donor area. There is no such thing as “scar-less” surgery, and any clinic claiming scar-free surgery exists is being purposely disingenuous and misleading. FUT leaves a linear incision line scar in the donor region. Healing is dependent upon physiology, but typically it is a very fine line of only 1-2mm with hair growing above, below, and even through it (for those who utilize a “trichophytic closure”). Patients can typically go down to a #3 on the buzzer (3/8th of an inch) before the incision line is visible. FUE leaves small “dot” scars scattered throughout the donor region. These are typically 1mm or less in diameter, and can be hidden very well when the excision sites are spread far apart and the patient has favorable skin/hair characteristics (the scars tend to heal lighter than the natural skin tone, so patients with fair skin and lighter hair color tend to heal very well). Patients can typically go down to a #2 on the buzzer (1/4th of an inch) before the dot scarring becomes visible. It is worth noting that scarring with FUE can become much more noticeable when larger sessions are performed. In these instances, the excision sites are placed much closer together and this forms both more visible scarring and can lead to a generalized thinned or “patchy” appearance in the donor. Both FUT and FUE scarring can be addressed with grafting and pigmentation camouflaging if ever needed in the future – though it typically is not necessary. However, patients must remember they will have visible scarring if hair transplantation is performed and typically the option to just “shave your head” is gone after the donor area is operated upon.
Donor Quality and Hair Characteristics
Donor quality and hair characteristics should be considered as well. Patients with dense, healthy donor areas can be suitable candidates for both FUE and FUT harvesting. They are less likely to note a “thinning” effect from the FUE harvest, and can easily hide the scarring from either method. Patients with less dense donor areas, however, need to carefully evaluate goals and proceed cautiously when considering either techniques. Sometimes patients with naturally sparse or “patchy” donor areas are better suited for conservative FUE. This technique provides the ability to “skip” around, and it may be easier to hide FUE scarring compared to a linear incision line in a thin donor area. However, these patients must keep in mind that they are still limiting their overall graft numbers by beginning with FUE. So FUT may still be better for patients who, despite a weaker donor supply, want better coverage on top and are willing to possibly grow the donor hair longer than average to hide the incision line.
The characteristics of a patient’s hair can play a role too. Patients with coarse, thick, wavy hair frequently have larger, heartier, and more robust follicular units. These thicker grafts tend to withstand the more traumatic FUE process better than patients with fine, straight hairs which are typically associated with smaller, more delicate, and less forgiving follicular units. However, this is not a guarantee nor a definitive factor in whether or not FUE will be successful. Sometimes patients with strong follicular units do not do well with FUE while others with seemingly more fragile grafts excel. The characteristics of the skin – both above and below the “surface” – also play a large factor as well.
Conclusions
Both FUT and FUE are refined, modern harvesting techniques which can produce excellent results when performed by the right team (led by an experienced hair transplant doctor) and for the right patient. Those with advanced hair loss or younger patients who need a large number of grafts or may need multiple surgeries over time are likely best suited by starting with FUT. Those who possibly only need a small number of grafts, possess certain donor characteristics, do not require large procedures in very visible areas, and may want to wear their hair as short as possible on the sides, could be good candidates for FUE. Patients should consult with a doctor capable and experienced in both techniques and together determine which approach is best.
